Article Text

Abstract
Introduction There have been recent reports of high vascular complication rates after the use of the Mynx vascular closure device (VCD). At our institution, vascular complications due to these devices have rarely been encountered. A study was undertaken to retrospectively compare angiographic abnormalities seen after femoral artery closure by both the Mynx and AngioSeal VCDs to provide further insight into the risks associated with VCDs.
Methods All adult patients who underwent deployment of either a Mynx or AngioSeal VCD and subsequently underwent repeat angiography within the next 30 days between 1 July 2010 and 1 April 2011 were reviewed. Two independent blinded radiologists compared blinded pre-procedure and follow-up femoral angiograms for the presence of pseudoaneurysm or other vascular abnormality. Hospital records were reviewed for major or minor complications of the groin site or femoral artery.
Results Thirty patients (31 angiograms) underwent vascular closure with a Mynx and 57 patients (69 angiograms) received an AngioSeal. The average time elapse until repeat femoral angiography was 6.2 days (range 1–21, median 5.5 days) in the Mynx group and 6.3 days (range 0–30, median 5 days) in the AngioSeal group. Two pseudoaneurysms and one minor stenosis were identified in the AngioSeal group. No angiographic abnormalities were seen in the Mynx group. No intraluminal filling defects were demonstrated on any of the follow-up femoral angiograms. One patient who received an AngioSeal developed a delayed minor groin site hematoma that did not require surgical intervention.
Conclusions Angiographic complications were seen in only 3% of patients after closure with Mynx or AngioSeal VCDs. There were no clinically significant groin site or vascular complications. These data suggest that both VCDs are safe for use after angiography with a low rate of femoral artery complications.
- Angiography
- cerebrovascular
- femoral artery
- vascular closure device
- aneurysm
- artery
- spinal cord
- subarachnoid
- thrombectomy
- catheter
- neck
- navigation
Statistics from Altmetric.com
- Angiography
- cerebrovascular
- femoral artery
- vascular closure device
- aneurysm
- artery
- spinal cord
- subarachnoid
- thrombectomy
- catheter
- neck
- navigation
Introduction
Vascular closure devices (VCDs) are commonly used to seal arteriotomy sites following endovascular procedures. At our institution, two VCDs are employed after neurointerventional procedures based on varying preferences among the three faculty members. The AngioSeal Evolution (St Jude Medical, St Paul, Minnesota, USA) closure device uses an intra-arterial bioabsorbable anchor that occludes the arteriotomy via extravascular compression applied by a suture and collagen seal. The Mynx (AccessClosure, Mountain View, California, USA) is an extravascular device that gained FDA approval in 2009. This system deploys a self-expanding water-soluble sealant without the need for vascular compression. This device biodegrades over several weeks and is marketed as inducing less scarring at the arteriotomy site than the AngioSeal device. We recently published a prospective single-blind study which showed a significant reduction in patient discomfort following Mynx closure compared with the AngioSeal device without any adverse events in either group.1 In this prospective study there were no complications related to groin closure with either device.
In contrast, some recent reports have implicated Mynx closure with a relatively high complication rate. Fields and colleagues observed an 18% incidence of intravascular Mynx sealant and 11% rate of pseudoaneurysm formation among 26 patients who underwent follow-up femoral artery angiography at a mean time point of 6 days following initial arterial closure.2 One patient with intravascular sealant underwent surgical exploration for near occlusion of the ipsilateral superficial femoral artery. Islam et al 3 published a similar case report of intravascular Mynx deposition that resulted in distal popliteal artery occlusion following percutaneous coronary angioplasty. The patient underwent emergency surgical removal of the intravascular sealant with successful recanalization.
At our institution we have rarely encountered any vascular complications related to either VCD. The aim of this study was to retrospectively compare angiographic abnormalities following femoral artery closure by both the Mynx and AngioSeal devices to provide further insight into the risks associated with VCDs.
Methods
The study institution is a high-volume neurointerventional center which performs over 1000 endovascular procedures per year. At the beginning of each procedure a femoral artery run is performed to image the arteriotomy site and the anatomy of the femoral artery. We exclusively use the Mynx and the AngioSeal devices at our center. VCDs are deployed at the conclusion of every procedure, with the choice of device based on faculty preference unless extenuating circumstances exist or the device manufacturer criteria for use are not met. VCDs are deployed by neurointerventional fellows on most occasions. Standard post-deployment care is set by the instructions for use of each device.
Our neurointerventional patient database was reviewed for all adult patients who underwent deployment of a VCD and subsequent repeat angiography within the next 30 days between 1 July 2010 and 1 April 2011. Patients without a VCD because of contraindications to the instructions for use were excluded from the study. Demographic information was recorded including gender and age as well as procedural information such as intraprocedural heparinization or the presence of periprocedure anticoagulant/antiplatelet agents (defined as aspirin or aspirin-containing medications, clopidogrel, ticlopidine or warfarin). Hospital records were reviewed for major or minor complications at the groin site or femoral artery.
Two independent blinded radiologists (JB and CR) compared blinded pre-procedure and follow-up femoral angiograms for the presence of pseudoaneurysm, minor (<50%) or major (>50%) vessel stenosis, the presence of intraluminal filling defects or no change in the vessel. The reviewers were unaware of the device that was used to close the arteriotomy. Patients with contralateral femoral access sites (and therefore angiograms of the opposite leg) and those without femoral angiography were identified and excluded from the statistical analyses.
Data were analyzed using SPSS. Independent-sample t tests and χ2 analyses were performed, with a chosen α level of 0.05 for statistical significance.
Results
Ninety-three patients with 111 repeat angiograms were identified during the study period. Nine patients had multiple repeat angiograms. Of these, 35 patients (38 angiograms) underwent vascular closure with a Mynx and 58 (73 angiograms) received an AngioSeal. Seven studies from the Mynx group and four studies from the AngioSeal group did not have follow-up femoral angiography of the previously accessed site during their second procedure and were therefore excluded, leaving 30 patients (31 angiograms) in the Mynx group and 57 patients (69 angiograms) in the AngioSeal group. The average time to repeat femoral angiography was 6.2 days (range 1–21, median 5.5 days) in the Mynx group and 6.3 days (range 0–30, median 5 days) in the AngioSeal group. Demographic, procedural and angiographic outcome data are presented in table 1.
Demographic, procedural and angiographic outcome data
Two pseudoaneurysms and one minor stenosis were identified in the AngioSeal group (figures 1–3). No abnormalities were seen in the Mynx group. No intraluminal filling defects were demonstrated on any of the follow-up femoral angiograms. One patient who received an AngioSeal device developed a delayed minor hematoma at the groin site that did not require surgical intervention. One pseudoaneurysm occurred in the setting of antiplatelet agents; the other pseudoaneurysm, the minor stenosis and the one minor hematoma at the groin occurred in patients who had not received systemic heparinization or antiplatelet agents.

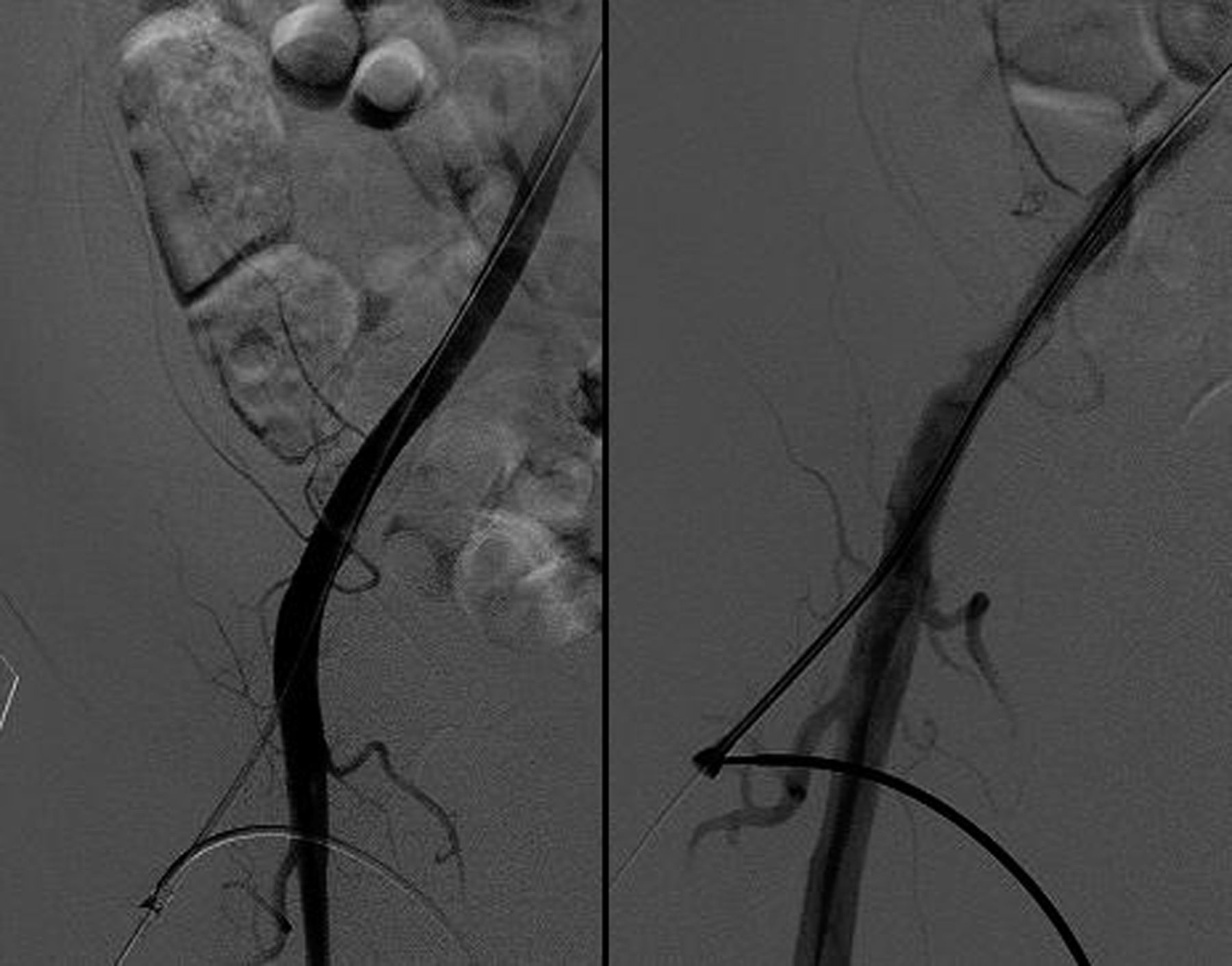
Pseudoaneurysm seen 1 day after AngioSeal deployment. Left panel: femoral artery angiogram before AngioSeal deployment. Right panel: femoral artery angiogram after sheath placement one day later.

A small pseudoaneurysm is seen distal to the sheath placement on repeat angiography 7 days after AngioSeal deployment.

{kind=link}
{kind=link}
{kind=link}
Mild femoral artery stenosis seen on repeat angiography 2 days after closure with AngioSeal. Left panel: femoral artery angiogram before AngioSeal deployment. Right panel: femoral artery angiogram after sheath placement 2 days later.
Discussion
In this blinded retrospective review of femoral angiograms after deployment of either a Mynx or AngioSeal VCD, only three angiographic complications were identified among 100 repeat angiograms (3%). The two pseudoaneurysms and one case of vessel stenosis all occurred in the AngioSeal group. One patient developed a clinically insignificant groin hematoma after AngioSeal. No patients required surgical intervention or additional treatment. Furthermore, there was no relationship between antiplatelet agents or heparinization with these complications. Although our study was not designed to record failure of device deployment at closure, we noted a very low angiographic complication rate with both the Mynx and AngioSeal devices and a 0% rate of clinically significant complications. Our data indicate that both VCDs are safe for use after angiography with a low rate of femoral artery complications.
The initial trial analyzing the safety and effectiveness of the Mynx device was published by Scheinert and colleagues in 2007.4 In this prospective multicenter single-arm trial, only one major vascular complication occurred that required blood transfusion (0.5%) among 190 patients undergoing either diagnostic or interventional procedures necessitating systemic heparinization. No device-precipitated complications were observed. The largest comparison study between the Mynx and AngioSeal closure devices was published in 2010 by Azmoon et al.5 In this retrospective study, 190 patients underwent femoral arteriotomy closure using the AngioSeal device and 238 patients underwent closure with the Mynx device following percutaneous coronary intervention. The incidence of major vascular complications (defined as retroperitoneal hemorrhage, pseudoaneurysm formation requiring surgical intervention and decrease in hematocrit by >3 g hemoglobin) was 2.1% for each group (not statistically significant). A higher incidence of device failure requiring manual compression was observed in the Mynx group than in the AngioSeal group (9.2% vs 3.7%). No long-term angiographic or clinical follow-up was available in this study.
Recently, Fields and colleagues observed an 18% incidence of intravascular Mynx sealant and 11% rate of pseudoaneurysm formation among 26 patients who underwent follow-up femoral artery angiography at a mean time point of 6 days following initial arterial closure.2 One patient with intravascular sealant underwent surgical exploration for near occlusion of the ipsilateral superficial femoral artery. A similar complication was reported by Islam and colleagues.3 It is unclear why Fields et al had such a high complication rate after Mynx deployment. The authors state that all individuals were trained in Mynx deployment and company representatives were present during many of the deployments. From a technical standpoint, closure with the Mynx requires more maneuvers than with the AngioSeal and therefore may be more susceptible to operator error. However, in our experience, vascular complications are relatively rare with either device. In our previous prospective study evaluating pain associated with closure, no clinically significant complications were demonstrated in either the Mynx or AngioSeal groups.
Based on the demonstrated safety and efficacy of both devices but the potential of higher device failure rates5 counterbalanced with decreased pain associated with the Mynx,1 we have adopted a general policy where patients under anesthesia undergo AngioSeal placement. However, patients who are awake receive Mynx closure to reduce their periprocedural pain. This appears to be a safe, effective and patient-centered means of performing vascular closure.
There are several important limitations to this study, including its retrospective nature and inability to determine the number of device failures requiring additional manual compression at the time of closure. Attempts were made to reduce reviewer bias by blinding the interpreting radiologists to the VCD used. Additionally, as this is not a randomized trial we cannot control for any potential selection bias that may be present. However, there were no significant differences in the demographic characteristics or antithrombotic medications of the cohorts. It should also be noted that minor groin hematomas are probably underestimated as these had to be documented in the hospital chart to be detected. Finally, this study does not compare angiographic outcomes after VCD closure with manual compression.
Conclusions
Angiographic complications were seen in only 3% of patients after closure using Mynx or AngioSeal VCDs. There were no clinically significant groin site or vascular complications. These data suggest that both VCDs are safe for use after angiography with a low rate of femoral artery complications.
Footnotes
-
Funding No funding was obtained for the completion of this manuscript. One-time non-monetary grant support had previously been received from Access Closure Inc (more than 2 years previously) for a different study.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by University of Florida IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.